A case of 23year Male with complains of paraparesis
This is a case of a 23year male patient who came to the OPD with the chief complaints of weakness of lower limbs bilaterally with other associated complaints.



I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
You can find the entire real patient clinical problem in this link here..
https://vaish7.blogspot.com/2020/05/medicine.html?m=1
Following is my view on this case-
Chief complaints in order of my priority are-
-bilateral lower limbs weakness
-vomitings
-gluteal abscess
-scrotal abscess
WEAKNESS-
-sudden in onset
-since 5 days
-associated with tingling and numbness
-has a history for fall during urination which might be related to the weakness
Now,what caused this sudden weakness of lower limbs bilaterally?
-It might be due to any arterial causes or an injury or Nervous system pathology.
Let’s see the patients general and systematic examination results-
General examination:
Pallor absent
Icterus absent
No cyanosis clubbing lymphademopathy,Edema
Afebrile
Bp 120/80 mm hg
Pr 80 bpm
spo2 98%
Cvs s1 s2 hears no murmurs
Rs bae + nvbs hears
P/a soft, non tender
Cns conscious
speech-normal
cranial nerves intact.
MOTOR SYSTEM
Right. Left
Bulk: normal. Normal
Tone: ul. normal. Normal
LL. hypotonia hypotonia
Power rt. lt
ul. 5/5. 5/5
LL. 2/5. 0/5
Reflexes.
Superficial reflexes
Right. Left
Corneal. P P
Conjunctival P. P
Abdominal. P. P
Plantar Extensor Extensor
Deep tendon reflexes
Right. Left
Biceps. 2+ 1+
Triceps. 2+ 1+
Supinator. 3+ 2+
Knee 3+ 2+
Ankle. 3+ 2+
jaw jerk. 1+. 1+
ankle clonus present. absent
Primitive reflex -absent
Involuntary movements - absent
SENSORY SYSTEM - normal
CEREBELLUM
titubation - absent
Nystagmus- absent
Intensional tremors - absent
Pendular knee jerk - absent
Coordination test -normal
MENINGIAL SIGNS
Neck stiffness - negative
Kernigns sign - negative
Brudzinkis sign - negative
Now, according to the given data above we can rule out arterial causes like varicose veins and peripheral artery disease which are the two most common arterial disorders that cause weakness of lower limbs.
Injury can also be ruled out as there was no history of trauma before
This leaves us with the nervous system disorders -
-from the data above the patients is hypotonic and hyoreflexes along with paraplegic which might be LMN lesions.But when X-ray abdomen was done it showed psoas muscle abscess along the left T4 and T5by which we can rule out LMN lesions and attribute it as paraparesis.
VOMITINGS-
-non-projectile ,non-bilious food particles
-5 days back with 2-3 episodes per day
Now non-projectile vomitings mainly incldiactes towards meningitis but the meningeal signs are all negative as mentioned above.Hence meningitis can be ruled out!
Now what caused these non-projectile vomitings?
ABSCESSES-
Gluteal abscess -5 months ago- operated
Scrotal abscess- 20 days back -10 days ago incised and drained.
What generally causes gluteal and scrotal abscess?
Mostly infection associated with streptococcal and staphylococcal bacteria cause these abscess but Mostly even in cases of HIV, our patient has a history of multiple sexual partners so hiv is possible .
-but HIV test Was negative
But in the above article there is a similar condition as our patient in relation to the abscess.
So based on the above article I can conclude that this gluteal and scrotal abscess is an extension from the psoas abscess which was the primary abscess.
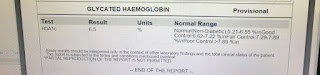
INVESTIGATIONS Reports-
There is significant enhancement which represents meningeal enhancement or exudates and following lesions in mri with multiple nodules in pulmonary apices suggest of pulmonary kochs and disseminated tuberculosis.
So now the Patient has tuberculosis but without any classical findings which can also be linked to his history of multiple sexual partners.
Based on the above finding we can conclude the following-
-Anatomical site involved-at level of T4 and T5 but not sure if other levels are involved are not because patient has both UMN AND LMN signs.
-pathology is due to disseminated TB which caused the abscess.
CURRENT TREATMENT OF THE PATIENT-
1)T.ATT 3 tabs/day fdc
2)T.Benadon 40mg/od
3)T.pregabalin 75mg/po/h/s
4)OINT.MEGAHEAL FOR LOCAL APPLICATION
5)SITZ BATH WITH BETADINE TID
6)FREQUENT CHANGE OF POSITION
Other treatment plans may include-
-intiate DOT

Comments
Post a Comment