"A patient centered approach to Alcohol Withdrawal, Peripheral Polyneuropathy and Polycythemia
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
You can find the entire real patient clinical problem in this link here.
The following case discussion can also be viewed from the link below
Following is the view of my case-
A 46year old male patient came to the opd with the chief complaints of pain abdomen since 4 days associated with vomiting since 4 days and loss of appetite since four days !
History of presenting illness-
Patient was apparently asymptomatic 6 years ago when he developed sudden involuntary movement of both upper limbs and later followed by both lower limbs with loss of consciousness and frothing .
-then he developed withdrawal seizures whenever he doesn’t take alcohol and seizures doesn’t occur after he consumes alcohol
-No medication used for seizures
-developed pain abdomen in the right upper quadrant which is of burning type,non radiating 4 days back which was insidious in onset and gradually progressive and it was asscociated with vomiting which was bilious nd non-blood stained and non-projectile.2-3episodes per day
-not associated with any loose stools
-loss of appetite since 4 days
Not a K/C/O DM, HTN, TB, CAD, Asthma
Mixed diet.
Disturbed sleep.
Loss of appetite since 1 week.
Known alcoholic since 17 years 90ml whiskey (OC) per day.
Tobacco chewer since 22 years.
Regular bowel and bladder movements
No known allergies.
No significant family history.
General Examination
Patient is conscious, coherent & cooperative.
Vitals
BP 110/70 mm Hg
PR 82 bpm
RR 19 cpm
SpO2 98% at RA
Afebrile
Icterus +
Palpebral conjunctiva appears red.
No signs of Pallor, Cyanosis, Clubbing, Generalized lymphadenopathy, Pedal edema
CVS
No visible pulsations
S1,S2 heard,loud P2
RV type of apex (diffuse)
Parasternal heave +
RS
BAE+
AP 25cm, TV 20cm
Chest expansion appears to be Rt>Lt, but all areas are expanding equally.
Percussion -
P/A
Soft.
Tenderness in the right hypochondrium, epigastrium and umbilical region.
No engorged veins & no organomegaly
Tympanic note on percussion.
Bowel sounds +
Abdominal circumference - 74cm
CNS
Tone
Normal in both upper limbs.
Hypotonia in both lower limbs.
Power - 4/5 in all limbs
Reflexes. Right. Left
Biceps. 3+. 3+
Triceps 2+. 3+.
Knee. absent. absent.
Ankle. 2+. 2+.
Plantar. Flexor. Flexor
Romberg test - Positive
Vibration
Both LL - 8 sec at ankle
Both UL - 8-10sec at wrist
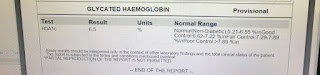
Investigations-









So now according to the blood report he has a high heamoglobin levels of about 19gm/dL which indicates polycythemia.
Polycythemia refers to an increase in the number of red blood cells in the body. The extra cells cause the blood to be thicker, and this, in turn, increases the risk of other health issues, such as blood clots.
So my questions for the following case are-
-what caused the polycythemia?
-what type of polycythemia?
-if it is polycythemia then why is there thrombocytopenia?
-are the seizures due to alcohol withdrawal or due to some underlying cns pathology?
-what caused the abdominal pain and vomitings ?
-why the serum alkaline phosphatase levels are increased along with elevated bilirubin and blood urea?
-does the patient have liver pathology that is effecting this heamoglobin levels and causing polycythemia?
-can alcohol itself directly cause polycythemia?

Comments
Post a Comment