Long case for practical exam
A 60 year old male patient, resident of Narketpalli, farmer by occupation, came with chief complaints of
- Shortness of breath since 2 months
- Cough with expectoration since 2 months
- Pedal edema since 2 months
- Fever since 2 months
History of presenting illness:
Patient was apparently asymptomatic before 2 months,
- then developed grade IV shortness of breath which increases on lying down.
- Cough with expectoration which is white in colour, non blood stained, non foul smelling.
- Bilateral pitting type below knee pedal edema.
- Fever which was insidious in onset, low grade developed two days after shortness of breath and cough started, not associated with chills and rigors. Relieved on taking medication.
No H/o chest pain , palpitations, decreased urine output , blood in urine, burning micturition.
Past history:
K/C/O Hypertension since 1 year, diagnosed on presenting with loss of consciousness and fatigue. He has been on medication since.
K/C/O CKD since 1 month
Not a K/C/O diabetes mellitus, thyroid abnormalities, TB, epilepsy, bronchial asthma, CVS disorders.
H/O surgery for appendicitis 8-9 years back and surgery for bowel perforation 5-6 years ago.
Personal history:
Diet: mixed
Appetite: reduced
Sleep: adequate
Bowel and bladder movements: regular
Addictions:
- smoking chutta 3/day since 18 years of age
- alcohol consumption since 18 years of age, 2-3 bottles/day of sara, Kallu or rum.
Family history: no significant family history.
General examination:
Conscious, coherent, and cooperative.
Thin built and moderately nourished
Pallor +, no icterus, cyanosis, clubbing, lymphadenopathy
Bilateral pitting type below knee edema present.
Central dialysis line present



Vitals:
Temperature: afebrile
PR: 100 bpm
BP: 186/120 mm Hg
RR: 38/min
Systemic examination:
CVS: S1, S2 heard. No murmurs. Apex beat at 5th intercostal space lateral to the mid-clavicular line.
Respiratory system:
- Shape of the chest is normal. Trachea in the central position. Apical impulse not visible. Movement of the chest with respiration reduced. No usage of accessory muscles or intercostal in drawing. No engorged veins, sinuses, scars, subcutaneous nodules, or swellings. Pulsation seen in the 3rd intercostal space in the mid clavichord line
- On palpation: no local rise of temperature or tenderness. Trachea is central in position. No expansion of chest elicited. Symmetry of the chest is normal.
- On percussion: dull note in the infra axillary and infrascapular region on the left side.
- Auscultation: BLAE +, NVBS, crepts heard in the left infra-axillary and infra-scapular regions.


Abdominal examination:
- on inspection, a midline globular swelling of size of a small orange above the umbilicus is seen. Surface is smooth with a longitudinal scar and hair on the skin over the swelling. Swelling moves with respiration.
- On palpation, no local rise of temperature and no tenderness elicited. No organomegaly. Inspection findings confirmed. Swelling is soft in consistency, no fluctuation elicited.
CNS:
- Higher mental functions-normal
- Cranial nerves- intact
- Sensory system- normal
- Motor system- normal
- Meningeal signs- absent
- Cerebellar signs- absent
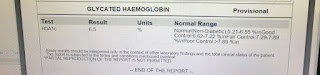
Investigations:
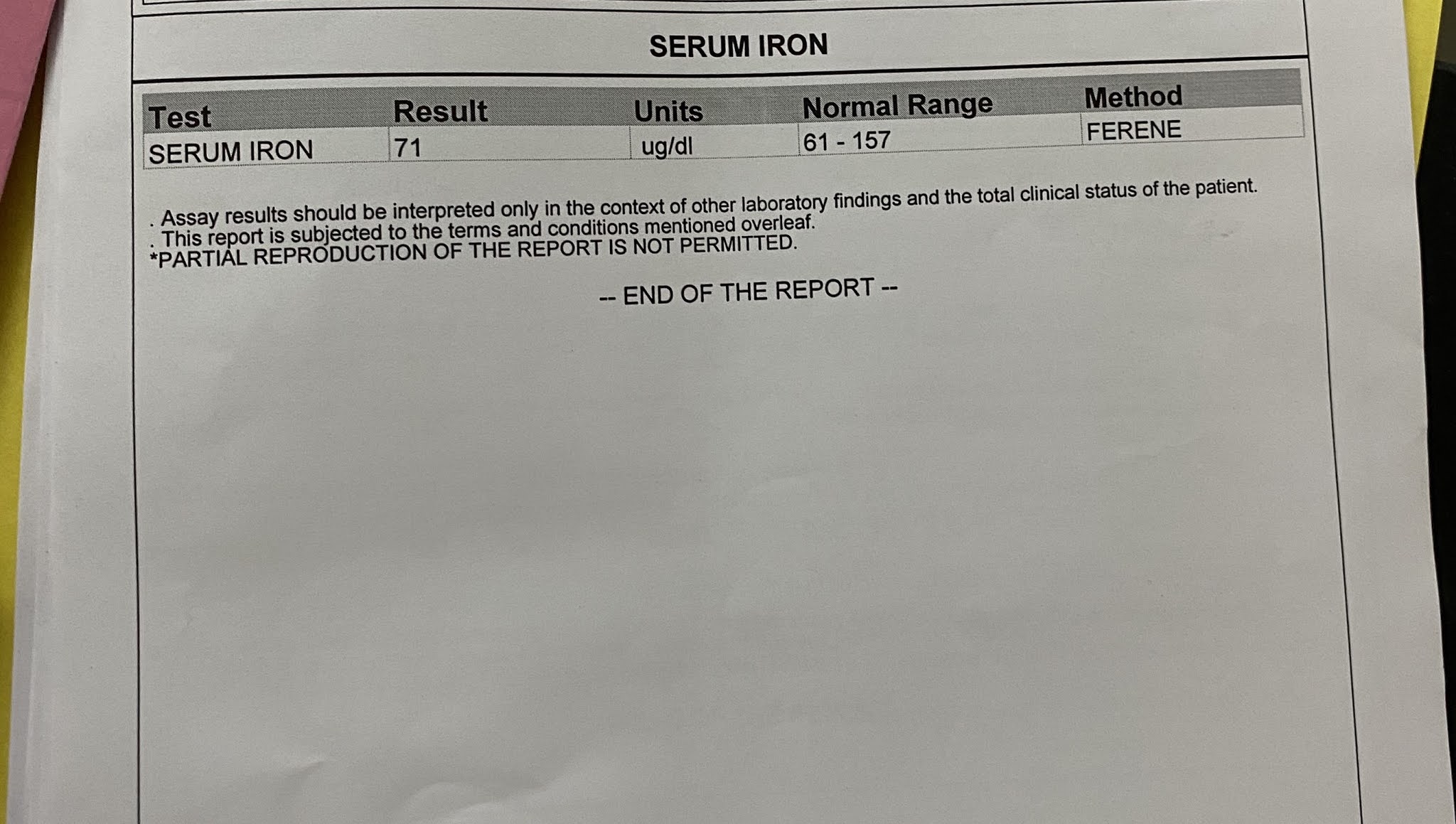







Differential diagnosis-
Chronic kidney disease with heart failure associated with hypertension and anemia
TREATMENT-
- TAB Lasix 40 mg PO/ BD

- TAB Nodosis 500 mg PO/BD

- TAB Shelcal CT PO/OD

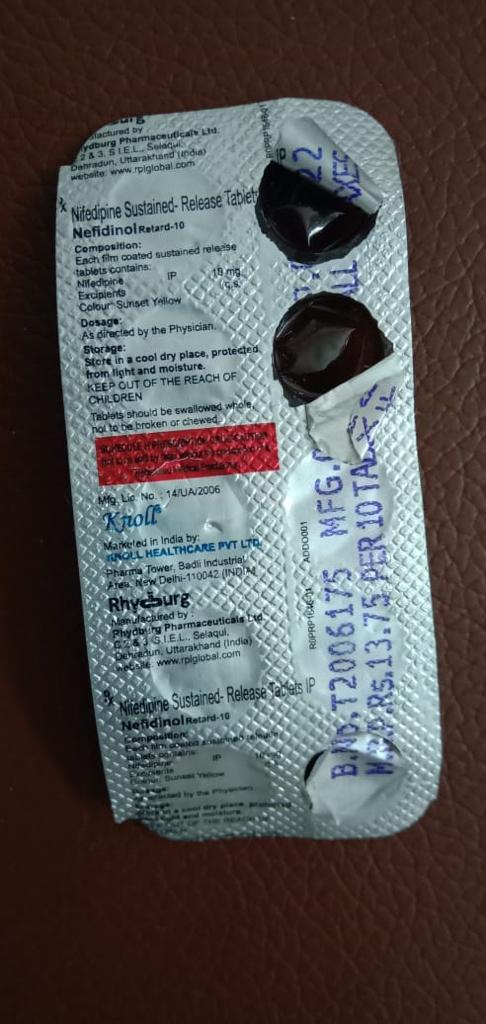
Tablet-nifedipine-10 mg thrice daily
Dialysis:
Patient underwent 10 sessions of dialysis since admission


Comments
Post a Comment